Fight CRC and Komodo Teamed up To Look at Time-to-Biomarker Testing and Treatment in Newly Diagnosed Patients
In recent years, advocacy organizations have made huge strides in bringing awareness to colorectal cancer (CRC). As the fourth most prevalent cancer in the U.S. and the second-leading cause of cancer-related deaths, CRC is now getting its due attention. Despite a decrease in overall incidence rates due to better screening and lifestyle changes, CRC still affects around 1.4 million Americans, and a noticeable increase in cases among younger people in recent years highlights the necessity for up-to-date research and targeted intervention strategies.
The journey from CRC diagnosis to treatment initiation is a critical period that significantly impacts patient survival and quality of life. Post-diagnosis biomarker testing can identify specific genetic mutations after diagnosis to predict treatment responses and enable a personalized approach. Access to early interventions, surgery, and chemotherapy are also crucial to improved outcomes. The treatment landscape is complex, however, influenced by socioeconomic factors, lifestyle risks, and family histories.
Fight CRC and Komodo Health have long collaborated to elucidate disparities in CRC diagnosis, care, and outcomes. This analysis of differences in time to testing and treatment in the U.S. was produced using Komodo’s MapLab™ solution, implementing several MapLab templates, including the Cohort Report to generate patient counts by age group and Patient Journey Analytics to gain insight into different patient journeys from symptom to diagnosis, treatment, and ongoing care. For this analysis, we looked at treatment initiation of both surgery and chemotherapy among newly diagnosed adult (age 18+) patients with a history of high risk for CRC, and those without. Additionally, we looked at the role of biomarker testing in influencing treatment timelines within these risk-defined cohorts and at delays through the lens of patient risk profile. Here is what we found:
1 in 3 patients with CRC received biomarker testing after their diagnosis, usually within a month of diagnosis.
We found that 37% of CRC patients received biomarker testing after their diagnosis and that the median time from diagnosis to biomarker testing was 27 days. This time to testing was similar across age groups, with patients ages 18 to 39 waiting the least amount of time, a median of 25 days, and patients ages 45 to 49 waiting the longest at 28 days.
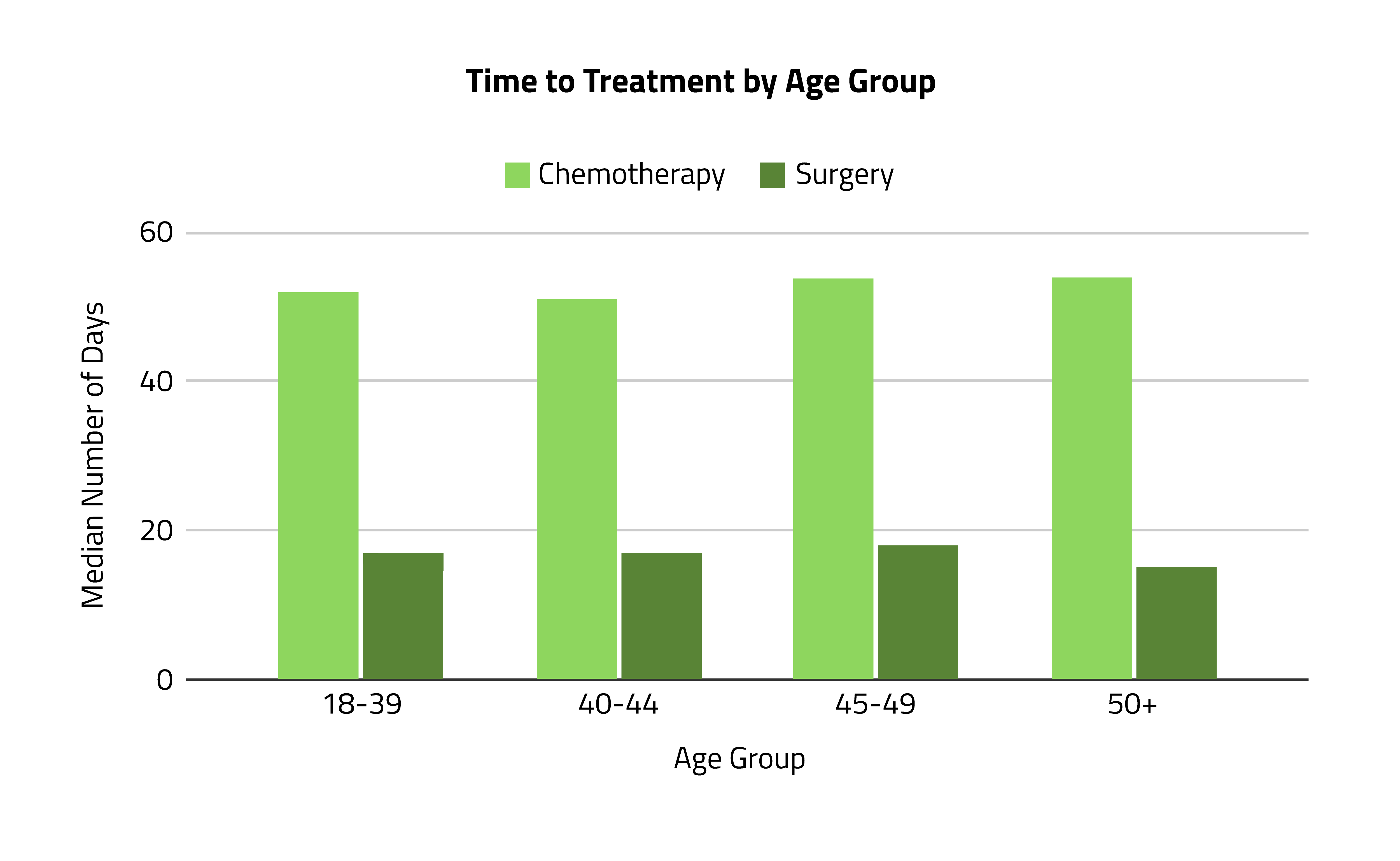
About 68% of patients received surgery or chemotherapy after their CRC diagnosis, initiated a median of 16 days after diagnosis.
Among patients with at least one year of data following their diagnosis, 68% had received treatment within that time frame. Of those treated, 96% received surgery and 59% received chemotherapy. These patients waited a median of 16 days after their diagnosis to initiate surgery and 54 days to initiate chemotherapy. Patients age 50+ had the shortest time to treatment for surgery (15 days), and patients ages 40 to 44 (51 days) had the shortest for chemotherapy.
Younger patients at high risk* for CRC received treatment slightly sooner after diagnosis than patients not at high risk.
Similar wait times overall were seen for time to treatment across patient risk profiles, with differences of 1 day or less. However, among the youngest cohort of patients ages 18 to 39, high-risk patients initiated treatment 4 days sooner than patients not at high risk (a median of 14 vs. 18 days).
Looking at time to biomarker testing, similar wait times were again seen across patient risk profiles overall, with differences of 1 day or less. However, a difference was seen among the youngest cohort (ages 18 to 39), with high-risk patients waiting 4 days longer for testing than those not at high risk (a median of 28 vs. 24 days).
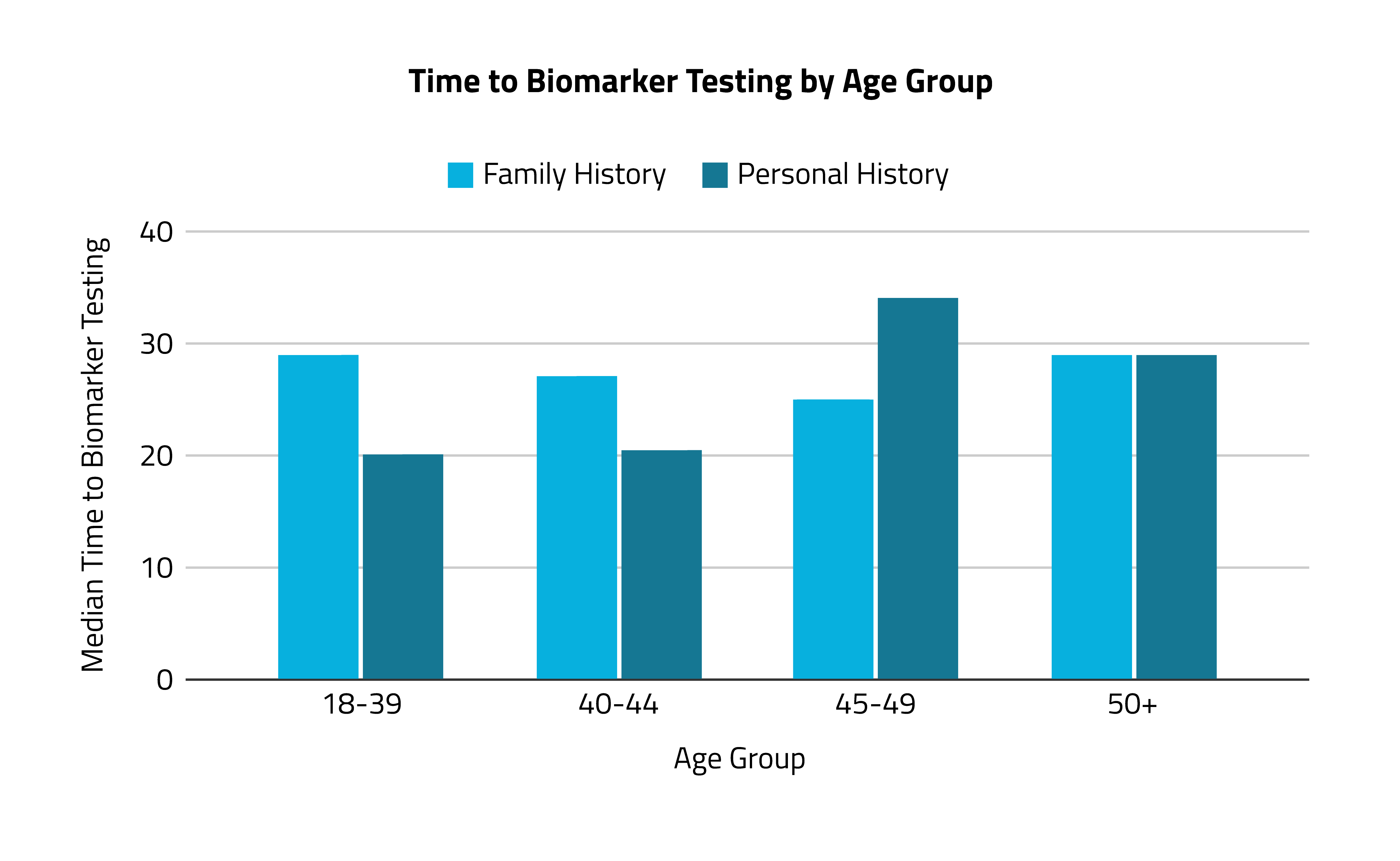
Younger CRC patients with high-risk personal histories received biomarker testing and treatment sooner than those with high-risk family histories.
When comparing all patients with a high risk of CRC due to family history vs. personal history, the overall median times to testing and treatment were the same for both groups. However, larger differences were seen among younger age groups: Patients age 18 to 39 with high-risk personal histories received biomarker testing a median of 9 days earlier than those with high-risk family histories, and they also received treatment 5 days earlier. Patients ages 40 to 44 with high-risk personal histories received biomarker testing a median of 6 days earlier than those with high-risk family histories, and they received treatment 8 days earlier.
These findings underscore both the complexity of the care timeline in CRC management and the importance of personalized healthcare strategies. They serve as critical insights for healthcare policymakers and practitioners, emphasizing the need for nuanced approaches that consider both demographic factors and individual risk profiles to optimize patient outcomes and equity in CRC treatment.
Analyses and insights like these are foundational in designing inclusive and effective healthcare policies that cater to the unique needs of diverse patient populations. By adopting data-informed approaches, healthcare systems can enhance care pathways, improve patient outcomes, and ensure equitable access to treatments. This analysis stresses the necessity of timely intervention in CRC treatment and showcases how leveraging data can revolutionize patient care, making it more personalized, efficient, and just. The move toward a data-informed healthcare system is pivotal for achieving a landscape where every patient receives timely and appropriate care.
For this analysis, “high risk” was defined as one or more of the following:
- Strong family history of colorectal cancer or certain types of polyps
- Personal history of colorectal cancer or certain types of polyps
- Personal history of inflammatory bowel disease
- Known family history of familial adenomatous polyposis or Lynch syndrome
- Personal history of radiation to the abdomen or pelvic area
Check out Komodo’s past collaborations with Fight CRC on diagnosis, care, and outcomes.


