
Heart disease is an equal-opportunity killer — male, female, Black, White, Hispanic, urban, and rural. As the leading cause of death in the U.S., accounting for some 695,000 deaths each year, heart disease affects virtually every demographic group — and every family — in America. Within that broad swath of demographic, socioeconomic, racial, and ethnic profiles, however, there are some very noteworthy variations. One of the most significant is geography. A recent study supported by the National Institutes of Health (NIH) found that adults living in rural areas of the U.S. have a 19% higher risk of developing heart failure compared to their urban counterparts. For Black men living in rural areas, that gap is even larger.
These findings follow a well-worn path of research suggesting that people living far outside the orbit of large, predominantly city-based academic medical centers often face barriers to care and worse outcomes than those with easier access to care. The findings also raise an important question about the conventional approach that Medical Affairs teams have taken for decades to identify and engage with providers: key opinion leader (KOL) research. This approach, which is key to a better understanding of real-world perspectives on different therapeutic areas and helps guide clinical development programs, is almost entirely focused on outreach at big teaching hospitals.
Flipping the Old-School KOL Workflow
That’s a problem when the majority of patients being treated in a particular therapeutic area receive care at smaller community hospitals, emergency departments, and primary care offices dotted throughout the country. Until recently, there was no practical way for Medical Affairs teams to efficiently identify and engage with these rural providers. While providers working in academic centers are routinely publishing and speaking at medical congresses and conferences, leaving a breadcrumb trail of evidence, those outside academia and large teaching hospitals spend more time treating actual patients and seeing the real-world impact of care.
 Now however, with advances in real-world evidence (RWE) and powerful tools like the suite of solutions built atop Komodo’s Healthcare Map™, Medical Affairs teams can quickly and easily identify providers not by how many articles they’ve published but by how many patients they are seeing with specific diagnoses and patterns of symptoms and treatments. This fundamental flip in the workflow — from targeting providers based on citations to targeting them based on patient reach and frequency — is dramatically altering how Medical Affairs teams approach different therapeutic areas. For conditions like heart disease, where the disease burden is nationwide, the approach makes it possible to close critical gaps in care.
Now however, with advances in real-world evidence (RWE) and powerful tools like the suite of solutions built atop Komodo’s Healthcare Map™, Medical Affairs teams can quickly and easily identify providers not by how many articles they’ve published but by how many patients they are seeing with specific diagnoses and patterns of symptoms and treatments. This fundamental flip in the workflow — from targeting providers based on citations to targeting them based on patient reach and frequency — is dramatically altering how Medical Affairs teams approach different therapeutic areas. For conditions like heart disease, where the disease burden is nationwide, the approach makes it possible to close critical gaps in care.
Identifying Gaps in Care for A-Fib Patients
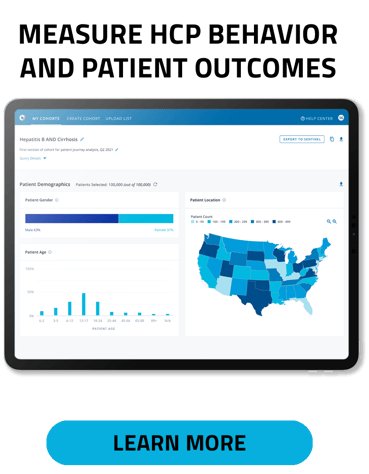
For example, we recently worked on a project with a Medical Affairs team tasked with expanding its universe of providers who treat patients with A-fib, a high risk of congestive heart failure, and vascular disease. Traditionally, the team would prioritize outreach to academic centers, but moving beyond legacy approaches, they wanted to expand their understanding and targeting of providers who saw many untreated A-fib patients both in and outside of large centers. By using our Prism solution to track specific diagnosis codes and patterns of care, we identified over 400,000 healthcare providers (HCPs) currently treating this patient population. Nationwide, that works out to an average of 2 patients per provider. More importantly, though, we were able to drill down into this patient population to find that just 27% of all HCPs had more than 60% of patients who were untreated for A-fib. For some providers, more than half of their patients — who are at the highest risk for heart failure or stroke — are not receiving care for their underlying condition.
Transforming Provider Engagement
While those results may seem shocking, they are not unique. We routinely find major gaps when we dig into specific conditions and chart the standard of care against the real-world experiences of patients in the U.S. healthcare system. There are many reasons for this and no shortage of research examining why routine care is often not available, ignored, or deferred, but the fact that we can now analyze these examples at scale is a critical breakthrough. By arming Medical Affairs teams with the details they need to reach out to providers throughout the country and educate them on the resources that are available to them — and their patients — and spotlight the gaps in care that currently exist, we are making it possible to get closer to the root of the problem.
Learn more about how Komodo Health helps Medical Affairs teams to transform provider engagement.
Share this:



