Less time on the groundwork. More time on the work that matters.
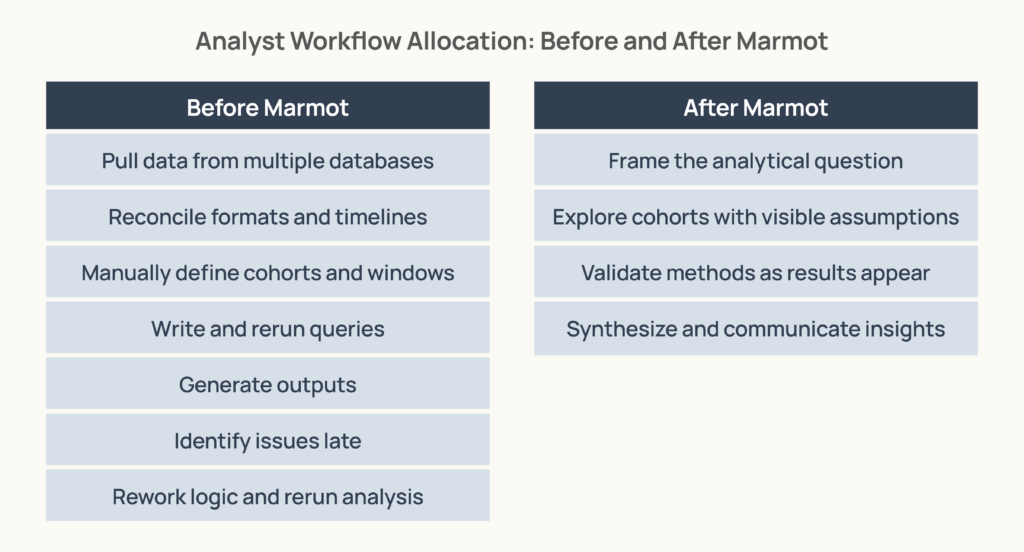
Healthcare analytics has always had a hidden tax: the work before the work — the heavy lifting of prepping data and validating logic that consumed most of an analyst’s time before any real analysis could begin.
AI is now compressing that groundwork. By handling the technical tasks that used to take weeks, AI allows the analyst’s value to move up the stack. As the time spent building manual outputs shrinks, the focus moves to what matters most: framing the right questions, interpreting the results, and turning data into decisions that people can trust.
From Artifacts to Insights
When the groundwork is laid faster, the analyst’s role shifts from building artifacts to providing essential context. Healthcare data rarely yields meaning in isolation; it requires a grasp of coding quirks and clinical nuance that automated systems can overlook. Without this expert layer, the output is just data, not a decision.
AI acts as a force multiplier, not just by compressing prep work but by serving as a partner in exploration. It can test multiple hypotheses in parallel to surface patterns that are nearly impossible to find manually. This allows the analyst to show up as a true thought partner who ensures the team is asking the right questions.
Ultimately, AI expands the scope of what can be discovered, but analysts ensure that those discoveries are grounded. They validate the assumptions and translate complex signals into a story that stakeholders can trust.
Case Study: Uterine Cancer Diagnostic Follow-Up in Marmot™
For a recent analysis, we wanted to know how often women received timely diagnostic follow-up after clinical signals that warrant uterine cancer screening and how that follow-up was broken down across different populations.
What we asked Marmot:
- Identify women age 50 and older with an initial presentation consistent with uterine cancer screening concerns
- Exclude patients who have undergone a hysterectomy or recent hormone replacement therapy
- Check whether they received a transvaginal ultrasound or endometrial biopsy after the initial signal, and measure how long it took
Marmot translated the request into a working population definition, applied the exclusions, and built the follow-up windows based on its knowledge of the therapeutic area.
What Marmot Performed
- Identified a screening-relevant population from claims patterns
- Isolated first-observed screening signals using lookback logic
- Applied exclusions for patients outside the relevant group
- Constructed diagnostic follow-up windows
- Calculated evaluation status, time to first procedure, and screening modality
- Examined where follow-up rates differed across demographic groups
- Stratified results by age group and race/ethnicity
Where the Analyst Stepped In
- Reviewed whether the identified procedures reflected clinically sound uterine cancer screening pathways
- Confirmed that the exclusions narrowed the population appropriately
- Interpreted time-to-evaluation patterns against benchmark data
- Determined which findings were robust enough to share externally
The findings surfaced by this analysis — identifying where diagnostic follow-up breaks down and for whom — are precisely the kinds of insights that inform real clinical and policy decisions.
Marmot got us to these insights faster. The analyst made sure we could stand behind them.
Moving Beyond Generic AI
Most AI tools were not built for the unique complexities of healthcare data. They often lack an understanding of how claims records are structured, how cohorts are defined, and how a single coding choice can alter a study’s entire conclusion. The manual burden doesn’t disappear when context is missing; it simply shifts to the back end. Analysts are left to verify plausible-looking outputs and reverse-engineer assumptions after the work is already “done.”
When AI is built with healthcare context from the start, the dynamic changes. Because the system understands the underlying logic, assumptions surface during exploration rather than after. This frees analysts from a cycle of retrospective validation and allows them to spend their time interpreting results and driving the strategy forward.
Read the full analysis on uterine cancer screening, or check out a recent analysis on the shifting care patterns and the use of GLP-1s in polyendocrine metabolic ovarian syndrome (PMOS, formerly PCOS).
To see more articles like this, follow Komodo Health on X, LinkedIn, or YouTube, and visit our Resources Hub.


