As GLP-1 use expands across metabolic care, we examine how diagnosis and treatment patterns are shifting among patients newly diagnosed with one of the most common endocrine disorders in women of reproductive age.
Key Takeaways:
- GLP-1 use among patients newly diagnosed with Polycystic Ovary Syndrome (PCOS) without type 2 diabetes rose 6.7-fold between 2020 and 2024.
- Nurse practitioners wrote more GLP-1 prescriptions for this group than any other provider type, accounting for 28.0%.
- Most patients with PCOS who started on a GLP-1 had commercial insurance: 72.5% vs. 18.7% on Medicaid.
- Patients who started GLP-1s shortly after diagnosis had higher metformin use and fewer fertility procedures.
- Median age at PCOS diagnosis stayed the same — 28 — from 2020 to 2025.
Polycystic ovary syndrome (PCOS) — which was recently renamed polyendocrine metabolic ovarian syndrome (PMOS) affects up to 5 million women in the U.S., yet diagnoses are often missed or delayed, and managing the condition remains inconsistent. PMOS is an endocrine disorder with broader metabolic manifestations, which can include obesity, insulin resistance, acne, hirsutism, and elevated long-term risk of diabetes and cardiovascular disease. It’s also a leading cause of infertility.
Symptoms emerge gradually and are reported in a variety of care settings, which can delay recognition of the full syndrome. At the same time, clinical understanding of PMOS has broadened, with increasing attention to its metabolic features alongside its reproductive effects.
At the same time, GLP-1s are taking on a larger role in the broader metabolic treatment landscape. Originally approved for type 2 diabetes, with some brands later receiving approvals for obesity and obstructive sleep apnea, these drugs are also being prescribed off-label for a range of conditions. In PMOS, their presence raises questions about current use in real-world care and how treatment patterns may differ among patients who receive them. Emerging clinical literature has stirred interest in their relevance to many PMOS-related symptoms.
We used Marmot, Komodo’s healthcare-native AI platform powered by our Healthcare Map, to better understand diagnosis timing, treatment patterns, and GLP-1 uptake in real-world PMOS care. We analyzed U.S. claims data from more than 1 million female patients ages 12 to 45 with a newly observed and confirmed diagnosis of PMOS (E28.2) between 2020 and 2025. We used each patient’s first diagnosis in the analytic period as the index date. Patients with any history of PCOS or any evidence of type 2 diabetes during the full timeline of available patient data were excluded.
To better place GLP-1 use within the PMOS care pathway, we analyzed new prescriptions after the initial PMOS diagnosis. We tracked two longitudinal metrics: 12-month new GLP-1 initiation rates among newly diagnosed PMOS patients; and 12-month treatment patterns among patients who initiated a GLP-1 within 6 months of a new diagnosis vs. non-initiators.
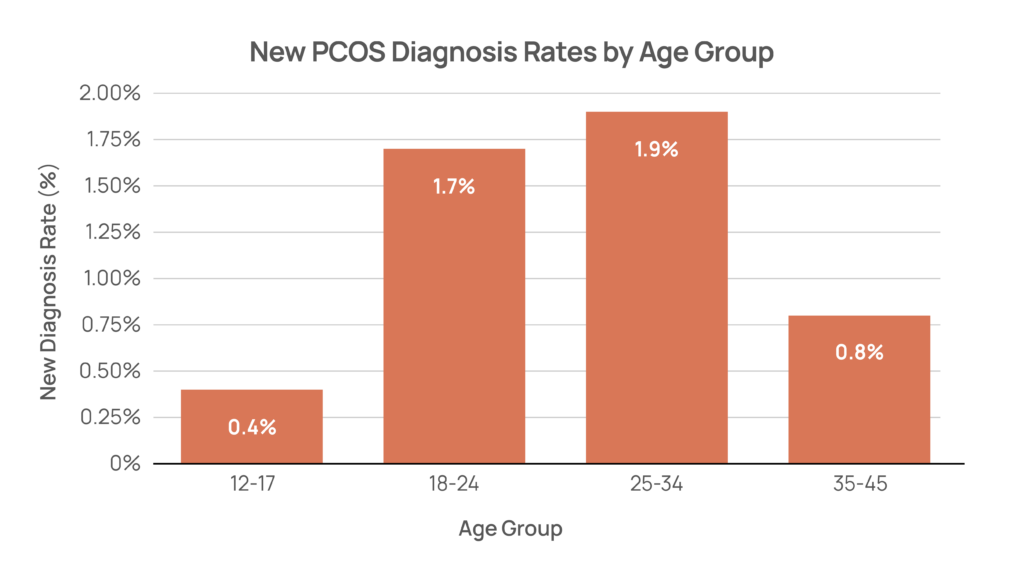
Age at diagnosis remained broadly stable from 2020 to 2025.
- The median age of PMOS diagnosis was 28 in every year of the analysis.
- New diagnosis rates were highest among women ages 25 to 34 (1.9%) and 18 to 24 (1.7%).
- 35% of newly diagnosed PMOS patients had hormonal birth control* use in the 2 years prior to diagnosis. Median age at diagnosis was nearly identical between patients with and without recent hormonal birth control use when controlling for birth year, suggesting no meaningful difference in diagnosis timing between the two groups.
*Hormonal birth control was defined using claims for oral contraceptives, the patch, vaginal ring, implant, hormonal intrauterine device, and injectable medroxyprogesterone acetate in the two years before diagnosis.
GLP-1 initiation increased about 6.7-fold among newly diagnosed PMOS patients and was concentrated among commercially insured patients.
- From 2020 to 2024, the share of GLP-1 initiation among patients newly diagnosed with PMOS who did not have type 2 diabetes increased from 1.1% to 7.3%.
- GLP-1 prescription rates had the greatest year-over-year growth in 2022 (+59%).
- GLP-1 initiation was driven primarily by nurse practitioners (28.0%), family medicine providers (22.4%), endocrinologists (16.3%), internal medicine providers (11.1%), and physician assistants (10.3%), while OB/GYN providers accounted for 5.5%.
- Commercial patients represented 72.5% of GLP-1 initiators and Medicaid patients, 18.7%.
- Wegovy and Zepbound accounted for 53.8% of GLP-1 prescriptions; Ozempic and Mounjaro accounted for another 31.5%, indicating substantial use of type 2 diabetes—labeled products despite exclusion of type 2 diabetes in the analytical cohort.

Early GLP-1 use aligned with more metabolic-oriented follow-up care and lower fertility-related and OB/GYN utilization.
- GLP-1 initiators had higher rates of metformin use (32.7% vs. 29.3%), endocrinologist visits (15.9% vs. 10.5%), and nutritionist/dietitian visits (7.7% vs. 5.8%) in the year following their PMOS diagnosis compared to non-initiators, while hormonal birth control use was similar in both groups (32.6% vs. 34.3%).
- GLP-1 initiators had lower rates of letrozole use (2.1% vs. 6.7%), clomiphene use (0.8% vs. 2.3%), fertility procedures* (4.7% vs. 13.4%), and OB/GYN visits (30.8% vs. 54.5%) in the year following their PMOS diagnosis compared to non-initiators.
*Fertility procedures were defined broadly to include claims related to insemination, embryo transfer, in vitro fertilization and related lab procedures, egg retrieval, fertility testing and monitoring, and other assisted reproduction services.

While treatment intent cannot be determined from claims data, GLP-1 use in newly diagnosed PMOS offers a useful window into how real-world care patterns are shifting in women’s health. Among patients with PMOS and related metabolic conditions such as obesity, these therapies may be prescribed for labeled metabolic indications while still shaping the broader PMOS care pathway. Monitoring GLP-1 use among women newly diagnosed with PMOS helps characterize a rapidly evolving treatment landscape and how these therapies may coincide with changes in downstream treatment patterns.
Komodo’s AI-powered analytics tools make it possible to evaluate shifting care patterns in large real-world populations with unprecedented speed, methodological consistency, transparency, and scale. That is especially important in treatment areas where real-world use is evolving rapidly.
About Marmot: This analysis was conducted using Komodo Health’s Marmot, the first healthcare-native AI analytics platform, built on the industry’s most comprehensive real-world data and designed to deliver transparent, verifiable insights at unprecedented speed. As Komodo’s recent published analyses have shown, tools like Marmot can help translate complex real-world treatment patterns into practical, decision-ready evidence, making it easier to understand how patients move through care as therapies, labels, and clinical practice continue to evolve.
To see more articles like this, follow Komodo Health on LinkedIn, YouTube, or X, and visit our Resources Hub.


