New nationwide analysis of nearly 800,000 women with postmenopausal bleeding between 2022 and 2023 reveals urgent gaps in care and striking inequities in who receives follow-up across geography, race, and age.
More than 90% of women with endometrial cancer — the most common form of uterine cancer — experience postmenopausal bleeding (PMB). While PMB is often caused by benign conditions such as vaginal atrophy or polyps, any vaginal bleeding that occurs 12 months or more after menopause warrants evaluation by a clinician. About 1 in 10 cases may be linked to endometrial cancer, making timely assessment critical. Clinical guidelines recommend transvaginal ultrasound and/or endometrial biopsy as first-line diagnostic tools to rule out malignancy or precancer and enable early, more effective treatment. Yet many uterine cancers are still diagnosed late, when treatment options are limited and outcomes are poorer. Adding to the urgency, rates of new uterine cancer cases rose by approximately 0.6% per year between 2010 and 2019. And rates of late-stage diagnoses and mortality also rose, especially among Black women and older patients.
Are opportunities for early diagnosis being overlooked?
We wanted to know how many women actually received the guideline-recommended PMB follow-up. We used Marmot™, our healthcare-specific AI analytics platform, to identify a cohort of women with newly diagnosed PMB, track their journeys, and discover how often opportunities for earlier endometrial cancer diagnoses were missed and any care disparities.
Specifically, we looked at a US cohort of women age 50 and older with newly diagnosed PMB between 2022 and 2023 and what percentage received either a transvaginal ultrasound or endometrial biopsy within 90 days of that diagnosis. We excluded women with any diagnosis or treatment history that might affect PMB, such as those receiving hormone-replacement therapy.
What we found revealed a major gap in adherence to national standards and striking disparities among insurance, race, and geography:
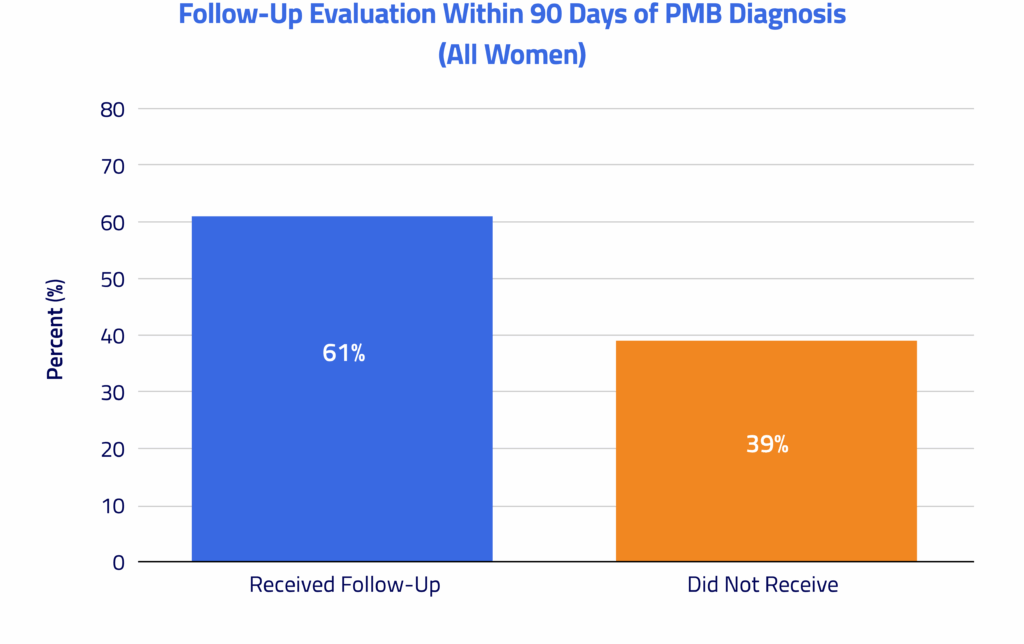
Only 61% of women with PMB received guideline-concordant diagnostic evaluation within 90 days.
Among nearly 800,000 de-identified patients in our cohort, 39% did not undergo a recommended diagnostic workup (transvaginal ultrasound or endometrial biopsy) within 90 days of their PMB diagnosis. When evaluation was pursued, it was delivered with significant promptness: 55% of patients were evaluated on the order date, 69% within one week, and 79% within two weeks, suggesting effective care coordination for many patients.
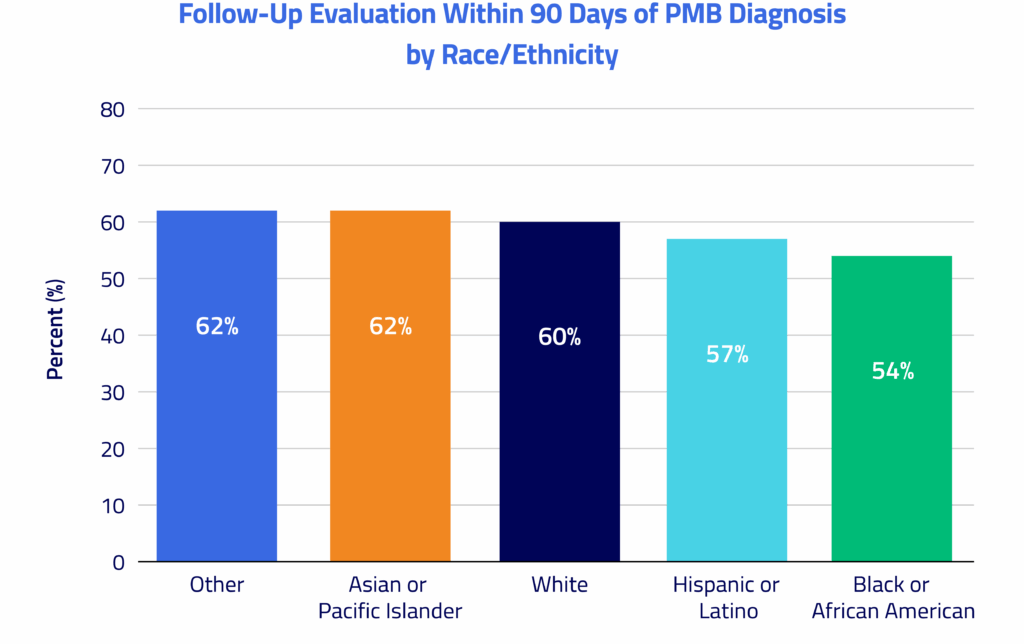
Black women had the highest rate of PMB (17 per 1,000) but the lowest diagnostic evaluation rate (57%).
This higher rate among Black women represents a 1.4x higher disease burden than among White women (12 per 1,000) but an 11% lower evaluation rate (64% in White women). Asian/Pacific Islander women also had high evaluation rates (64%) despite lower PMB incidence, underscoring racial inequities in how patients with this high-risk symptom are assessed.
Commercially insured women were more likely to receive guideline-concordant evaluation, with a 15% higher rate than publicly insured patients.
Approximately two-thirds of commercially insured women completed the recommended diagnostic evaluation within 90 days of initial postmenopausal bleeding diagnosis. Patients insured by Medicaid had a higher incidence of postmenopausal bleeding (12 per 1,000) than those insured by Medicare (9 per 1,000), yet they received the recommended diagnostic follow-up least often across insurance groups.
Diagnostic evaluation rates varied by 24 percentage points across states, from 50% at the low end to 73-74% in Wisconsin, Vermont, and Minnesota.
A clear regional pattern emerged: Northeastern and Upper Midwest states consistently showed higher evaluation rates, while Southern and Southwestern states, including Florida, Mississippi, and Oklahoma, showed the lowest rates. States with higher PMB incidence (e.g., Vermont at 17 per 1,000) generally also had higher evaluation rates, suggesting that diagnostic workup may partly track with underlying disease burden.
This analysis underscores the importance of strengthening adherence to clinical guidelines nationwide. By addressing existing gaps in evaluation and care delivery, we can help ensure more timely diagnoses and equitable outcomes across diverse patient populations.
To see more articles like this, follow Komodo Health on LinkedIn, YouTube, or X, and visit our Resources Hub.
About Marmot: This analysis was conducted using Komodo Health’s Marmot, the first healthcare-native AI analytics platform, built on the industry’s most comprehensive real-world data and designed to deliver transparent, verifiable insights at unprecedented speed.


