A real-world analysis of prescribing, access, and CPAP use following the FDA approval of Zepbound for obstructive sleep apnea
Key Takeaways |
|
A milestone in sleep apnea care
In December 2024, the U.S. Food and Drug Administration (FDA) approved tirzepatide (Zepbound) for the treatment of obstructive sleep apnea (OSA) in adults with obesity. The approval marked a milestone in OSA treatment: the first pharmacologic option shown to address contributing metabolic pathways of the condition rather than airway obstruction alone.
For decades, device-based therapies — most notably, continuous positive airway pressure (CPAP) — have been the cornerstone of OSA treatment. While effective, CPAP adherence remains a persistent challenge, and the therapy does not address the metabolic and inflammatory pathways that often contribute to OSA severity.
The FDA’s approval of tirzepatide also had broader implications for access. Expanding the labeled indication to include OSA opened the door to payer-supported access to GLP-1 therapy for patients with obesity-associated OSA, with the potential to reduce reliance on devices.
OSA affects roughly 30 million adults nationwide, and obesity is a major risk factor. Both conditions share overlapping metabolic and inflammatory pathways that can impede long-term health. OSA is associated with serious downstream risks, including hypertension, cardiovascular disease, type 2 diabetes, stroke, and cognitive decline, making early and effective treatment critical.
Tracking real-world adoption
To better understand real-world uptake, prescribing behavior, and the clinical impact of this label expansion, we used Marmot™, Komodo’s healthcare-native AI platform powered by our Healthcare Map®, to analyze claims data from nearly 20 million adults diagnosed with OSA.
We examined patients newly starting tirzepatide for initiation patterns before and after the December 2024 label expansion and changes in CPAP initiation and engagement. We also looked at overlapping CPAP prescriptions and signals for CPAP discontinuation, which was proxied by a six-month gap in CPAP-related claims — referred to as CPAP engagement (while this does not confirm clinical discontinuation, differences before and after approval provide meaningful directional insights).
The analysis quantified the size of the potentially eligible population, characterized prevailing treatment patterns, and assessed early adoption trends during the months following FDA approval of tirzepatide for OSA. The analysis focused on adults age 18 and over.
What we learned
GLP-1 use was historically limited in OSA treatment.
- Prior to label expansion, only 14% of patients diagnosed with OSA received any GLP-1 therapy, compared with 66% who received device-based treatment such as CPAP. When taking a longer view of patients’ medical histories (including before OSA diagnosis), GLP-1 exposure rose to 24%. This underscores the limited role that pharmacologic therapy historically has played in OSA management relative to devices.
- A meaningful portion of the overall OSA population likely meets labeled eligibility criteria for GLP-1s. Published epidemiologic estimates suggest that approximately 39% of adults with OSA have moderate-to-severe disease, and 43-54% of those patients meet criteria for obesity — the population that tirzepatide is now indicated for.
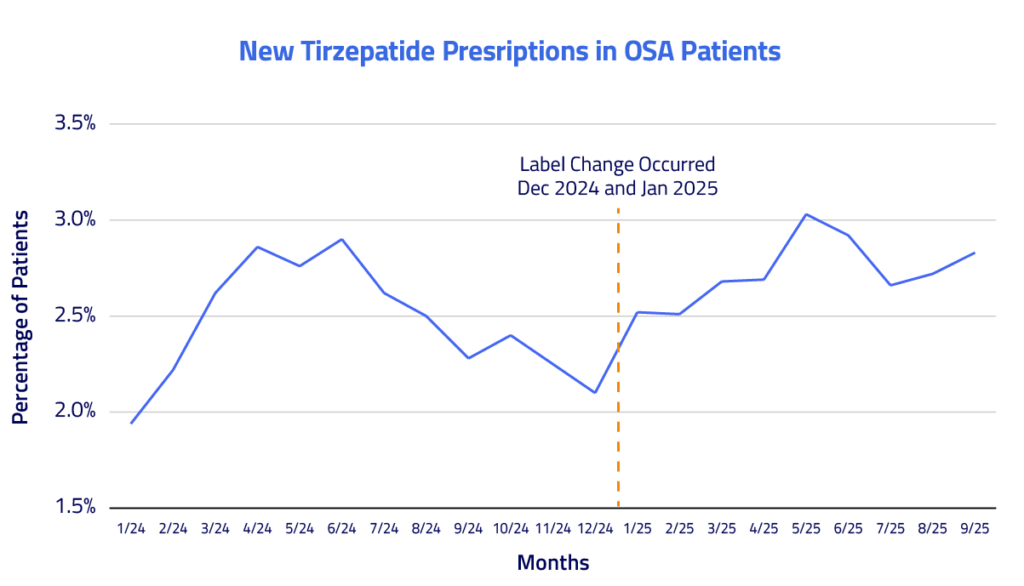
Tirzepatide uptake increased among OSA patients following label expansion.
- In the six months following approval (January–June 2025), new starts increased by 16% among OSA patients.
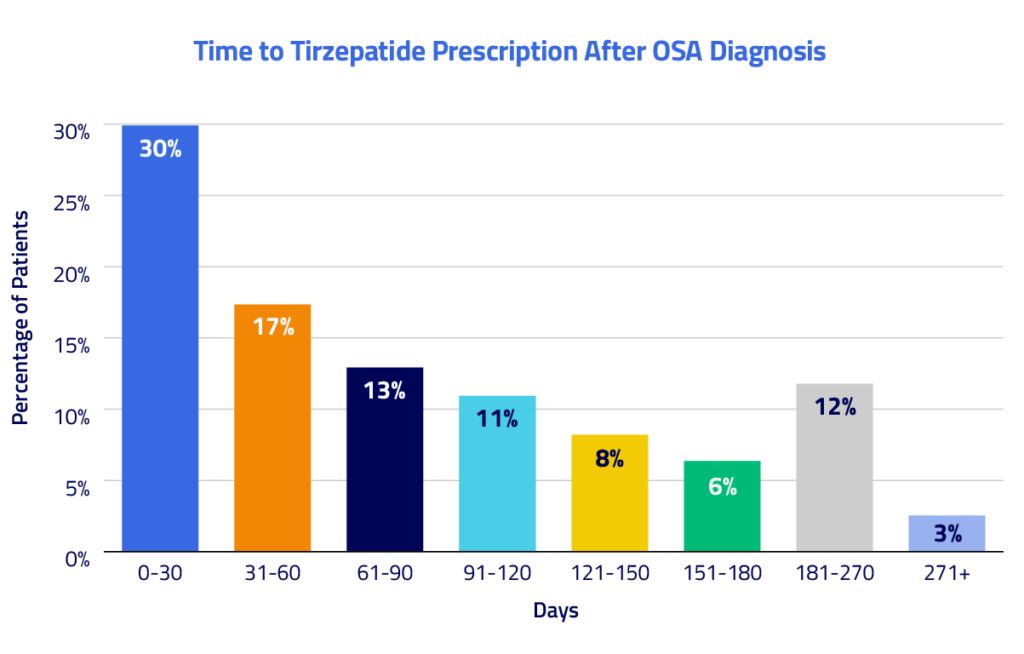
- Tirzepatide was often initiated early in the OSA treatment timeline. Nearly 30% of newly diagnosed OSA patients initiating tirzepatide did so within 30 days of their OSA diagnosis, and 47% initiated within 60 days. Only 3% initiated treatment more than 270 days after diagnosis. This may reflect the GLP-1 being introduced as an initial step in the treatment timeline rather than after prolonged device use.
Middle-aged adults accounted for the highest initiation rates. Adults ages 45–54 had the highest initiation rate (91 per 1,000 patients with OSA), followed by ages 35-44 (87 per 1,000). Rates were lowest among adults 75 and older (37 per 1,000).
OSA patients who received tirzepatide initiated CPAP therapy about 83% less often than those who did not receive the drug.
Among patients with OSA who had no prior CPAP use, only 4% of those who initiated tirzepatide went on to start CPAP therapy within six months, compared with 22% of those without GLP-1 exposure. This 83% relative difference indicates that tirzepatide is often being used early in the treatment pathway, potentially reducing reliance on first-time initiation of device-based therapy.
Tirzepatide initiation was associated with lower CPAP engagement among existing users.
Among patients with OSA who used a CPAP, 26% of those who initiated tirzepatide showed a six-month gap with no CPAP-related claims, compared with 15% of matched patients with OSA who did not receive the drug — a 75% relative difference. While a gap in claims cannot be interpreted as definitive clinical discontinuation, the difference suggests meaningfully lower engagement with CPAP-related services following tirzepatide initiation.
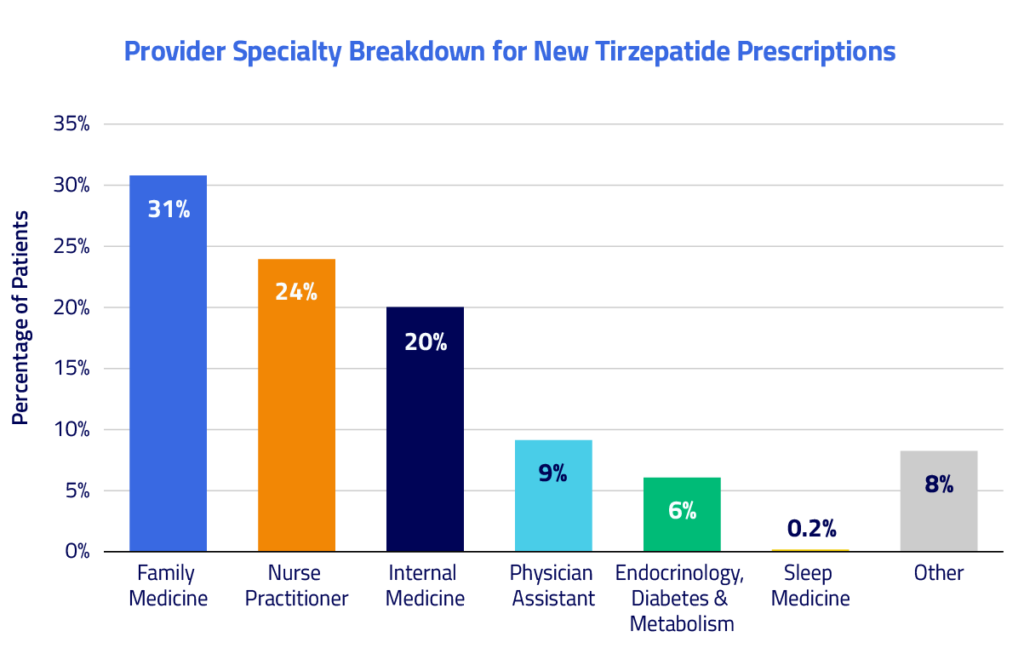
Tirzepatide prescriptions for OSA were most often written by primary care providers, with minimal involvement from sleep specialists.
- Family medicine physicians wrote 31% of tirzepatide prescriptions among patients with OSA, followed by nurse practitioners (24%), internal medicine physicians (20%), and physician assistants (9%). Endocrinology, diabetes, and metabolism specialists accounted for 6% of prescribing.
- Taken together, primary care and generalist settings accounted for approximately 84% of all new tirzepatide prescriptions, underscoring that prescribing is largely driven by frontline care rather than specialty services. In contrast, sleep medicine accounted for just 0.2% of prescriptions.
Translating regulatory change into real-world insight
These findings highlight how quickly regulatory approvals can reshape real-world care. Within months of FDA approval, tirzepatide was already influencing prescribing behavior, treatment timing, and reliance on CPAP among patients with OSA.
As new indications blur the lines between specialty-driven care and population-level treatment, stakeholders require visibility into how therapies are actually adopted and how they reshape downstream care. This analysis shows how real-world data analyses can enable teams to move quickly from regulatory change to insight, capturing early signals across diagnosis, prescribing behaviors, and care pathways on a national scale.
Translating regulatory milestones into practical understanding moves beyond market intelligence — it helps ensure that advances in therapy lead to clearer, more navigable care journeys for patients when it matters most.


