Examining the Impact of the COVID-19 Pandemic on the Use of DNR Orders, Highlighting Differences by Demographic
Key Takeaways |
|
In recent years, public awareness of do-not-resuscitate (DNR) orders has grown, further driven by the COVID-19 pandemic and more dialogue among healthcare professionals and public figures. More practitioners are speaking out about ethical considerations, patient autonomy, and the importance of informed decision-making about DNR status, especially in the context of serious illnesses and an aging population. This has prompted greater public understanding and engagement in end-of-life planning discussions.
The pandemic marked further shifts in healthcare decision-making, and DNR orders emerged as a critical social and ethical focus for certain patients and their families. But has that trend lasted? Recent research found that the use of DNRs increased among older patients during the pandemic, a period noted for a troubling amplification of existing racial and socioeconomic disparities in healthcare access. Black and Hispanic patients, already facing barriers to equitable care, were found to have experienced disproportionately higher mortality rates and were more likely to establish DNR orders during this period.
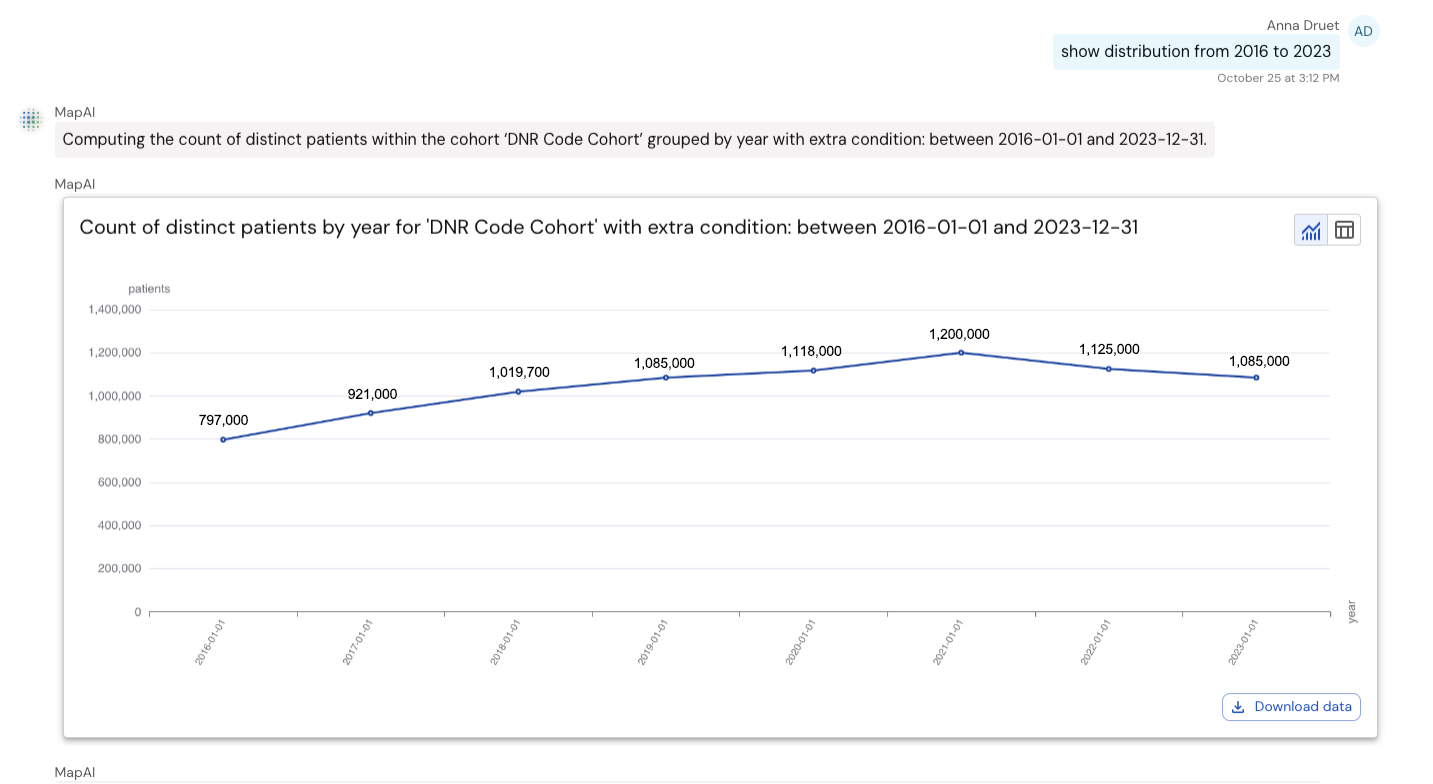
To further explore this and other trends in DNR order utilization (ICD-10-CM code Z66) on a larger scale, we used Komodo’s conversational analytics tool, MapAI™, and custom analytics built from the MapLab™ ecosystem. By examining patterns across age, gender, race, payer channels, and region, we sought a clearer understanding of how recorded DNR status has evolved over time and across diverse patient groups.
Here’s what we found:
Between 2016 and 2023, the number of patients with a DNR order increased by 36%.
An additional increase of 11% was seen during the peak of the COVID-19 pandemic, but numbers returned to pre-pandemic levels by 2023, indicating no lasting impact of DNR awareness brought by the pandemic era. As expected, DNR patients were predominantly age 65 or older (84%) and insured by Medicare (83%). DNRs were equally as common across genders.
The rate of DNRs varies widely by state — older adults living in Maine were most likely to have a DNR, and older adults in Florida were least likely.
After adjusting for the number of patients age 65+ by state, an average of 8% had DNRs across all states. Maine had the highest rate (15%) in the 65+ population, followed by New Hampshire (13%) and West Virginia (12%). The lowest DNR rate was found among older adults in Florida (4%).
Overall, White patients were 130% more likely than Black patients to have a DNR; however, Black patients had the biggest increase in DNRs during the pandemic.
MapAI generated raw numbers for patients of all ages who had a DNR — 70% identified as White, 9% as Black, 7% as Hispanic or Latino, 3% as Asian or Pacific Islander (AAPI), and 8% as Unknown. After adjusting for population by race and ethnicity, 8% of White patients age 65+ had a DNR — higher than the average of 5% across patients of color. However, during the pandemic, Black and Hispanic and Latinx patients had significantly higher increases in new DNRs — 12% and 7%, respectively, compared to just 3% for White patients.

This analysis highlights a strong and growing trend toward utilization of DNR orders and the pressing need to address race-based disparities in end-of-life care. While the growing prevalence of DNR orders signals greater awareness, the uneven distribution across certain populations and the disproportionate increase among those groups during the COVID pandemic should spark further investigation.
By leveraging MapAI and real-world insights from Komodo’s solutions, healthcare stakeholders have an opportunity to quickly and easily track trends as they unfold to both inform policy decisions that reflect on-the-ground truth and maximize the efficacy of interventions in reducing disparities — a key tenet of Komodo Health’s patient-focused mission.
To see more articles like this, follow Komodo Health on X, LinkedIn, or YouTube, and visit Insights on our website.


